Abel N. Onunu, MBBS, FWACP , and Emmanuel P. Kubeyinje, MBBS, FWACP, FRCP
Abstract
Background
There is a paucity of reports on vitiligo in sub-Saharan Africa.
Aim
To define the clinical and epidemiologic pattern of vitiligo in the Nigerian African.
Methods
We examined all new cases of vitiligo seen in the Dermatology Unit of the University
of Benin Teaching Hospital (UBTH) over a 14-year period: January 1985 to December 1998.
Results
Three hundred and fifty-one patients with vitiligo, representing 3.2% of new
dermatologic cases, were enrolled. The study group was made up of 153 males and 198
females, giving a sex ratio of 1 : 1.3. The peak incidence of vitiligo was in the second and third
decades of life, and the most common form of presentation was the localized focal type (77%),
followed by the segmental type (12.5%) and the generalized form (10.5%). Common sites
affected were the limbs (32%), trunk (23.8%), face (18.2%), head and neck (9.1%), and the
mucous membranes (7.4%). There was a positive family history of vitiligo in 18% of subjects and
3.4% had systemic diseases, such as diabetes mellitus (1.7%), anemia (0.8%), hyperthyroidism
(0.6%), and leukemia (0.3%).
Conclusions
Vitiligo on darkly pigmented skin is often a very striking disease. Our findings
show that the pattern of vitiligo is similar to that reported from other parts of the world. The high
level of social stigmatization is due to confusion with leprosy.
Introduction
Vitiligo is a specific acquired disorder of the skin, hair, and mucous membranes characterized by patches of depigmentation due to the complete loss of melanocytes. Occasionally, it involves other melanocyte bearing areas, such as the uveal tract of the eyes and retina.
Cosmetically, vitiligo is one of the most disfiguring of disorders, especially in deeply pigmented
skin, where the lesions are often very striking.It causes significant emotional distress, and in societies in which leprosy is endemic, vitiligo carries an additional burden of social stigmatization associated with most hypopigmented skin diseases.
There are three main patterns of presentation: a common generalized form, a segmental type that usually involves the dermatomes, and the localized focal type. The etiology is unknown, but autoimmune and neurogenic factors have been implicated. Self-destruction of the melanocytes by melanin precursors is also thought to play some role in the pathogenesis
of vitiligo.
Most large studies on vitiligo have been from North America, Europe, and the Indian subcontinent, with
only a few from Africa.The objective of this study is to present the features of vitiligo as seen in the University of Benin Teaching Hospital (UBTH), Benin City, Nigeria, over a 14-year period.
Patients and methods
The study population was made up of all consecutive patients with vitiligo, referred for specialist dermatologic consultation at the Dermatology Clinic, UBTH, over a 14-year period (January 1985 to December 1998). The Dermatology Clinic is the main referral center for skin diseases, serving a population of more than 800,000 residents in Benin City and its environs. The diagnosis of vitiligo was mainly clinical, with skin biopsy and histopathologic examination performed in doubtful cases to exclude leprosy. Details of the history and clinical pattern, as well as the presence of any other systemic diseases, were noted in each patient. Routine investigations were performed, including full blood count,
urinalysis, fasting blood sugar, serum electrolytes, urea, and creatinine levels. More sophisticated investigations for diseases of other organ systems were performed only when clinically indicated.
The treatment given to patients included topical psoralen with graduated exposure to sunlight, systemic corticosteroid combined with topical corticosteroid, systemic corticosteroid alone, or topical
corticosteroid alone.
Results
A total of 351 patients with vitiligo, representing 3.2% of new dermatologic consultations, were recruited during the study
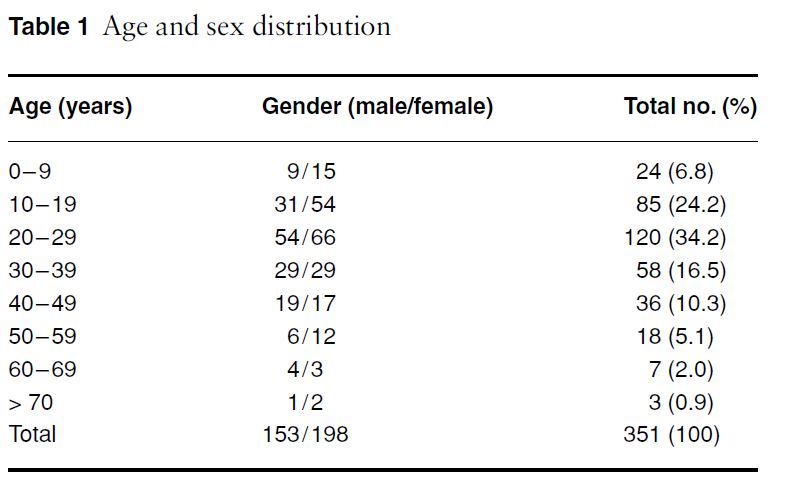
period. There was a slight female preponderance with 153 males and 198 females, giving a male to female ratio of 1 : 1.3. Vitiligo was seen in most age groups: the youngest patient was9 months old, and the oldest was 80 years old. The peak age incidence was in the second and third decade of life (Table 1).
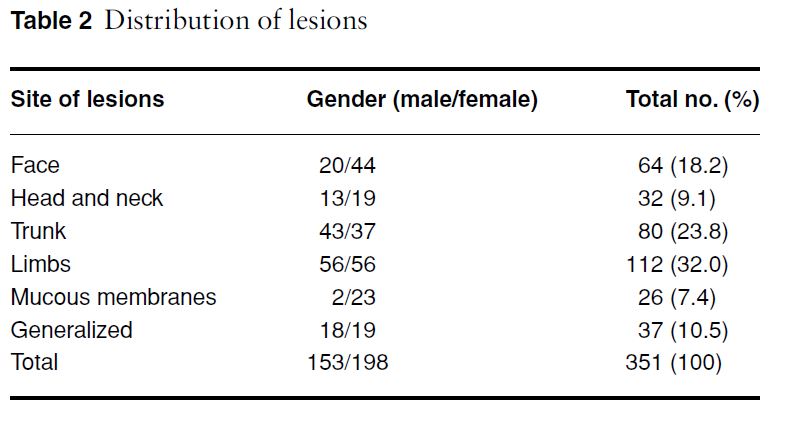
There was a positive history in 63 (18%) patients. Twelve (3.4%) patients had associated systemic diseases: six (1.7%) had diabetes mellitus, three (0.8%) had anemia, two (0.6%) had hyperthyroidism, and one (0.3%) had leukemia. The lesions were segmental in 44 (12.5%) patients, generalized in 37 (10.5%), and localized in 270 (77%). The most commonly affected sites were the exposed parts of the body, in particular the extensor surfaces of the limbs (32%), face (18.2%), and the head and neck (9.1%). The trunk was involved in 23.8% of patients, and 7.4% had lesions on the mucous membranes of the lips, vulva, nipples, and gingiva (Table 2). Subjects with lesions on exposed parts of the body experienced some social
stigmatization because of confusion with leprosy.
Worldwide, the average incidence of vitiligo is estimated to be about 1–2% (range, 0.14–8.8%) of the general population.The incidence in Nigerians in this study was 3.2% of new dermatologic cases. Similar rates have been reported from the Middle East and the Indian subcontinent, where the
darkly pigmented skin of the natives makes vitiligo more obvious.
Both genders are vulnerable to the disease. The slight female preponderance, similar to that reported in other studies, is believed to be the result of women being more sensitive to cosmetic disfigurement and therefore more likely than men to present for treatment.
A study in Ibadan, Nigeria of 64 cases of vitiligo found no history of the disease in families; however, in our series, 18% of subjects had a positive family history of vitiligo, which is similar to the findings from other parts of the world (6.25–38% of patients with a family history of vitiligo). The inheritance pattern is not fully established; some studies seem to suggest an autosomal dominant gene with variable expression and incomplete penetrance.
Most of our patients had lesions on exposed parts of the limbs (32%), face (18.2%), and head and neck (9.1%). Other parts involved were the trunk (23.8%) and the mucous membranes (7.4%). The ratio of the various clinical types of vitiligo, namely focal, segmented, and generalized, was similar to
that found in other regions of the world.
Vitiligo was associated with other systemic diseases in 3.4% of subjects. The
incidence of thyroid disease in vitiligo has been reported to vary from 1.3 to 30%. The incidence of thyroid disease in this study was 0.6%, probably because only those with clinical
features were screened.
The suggestion by Ochi and DeGroot that vitiligo associated with thyroid disease classically
involves the palms and soles was not evident in our two patients. Diabetes mellitus is thought to occur in 1–7.1% of patients with vitiligo.
Only 1.7% of our study subjects had diabetes mellitus; this was no different from the prevalence
of diabetes mellitus (1.7%) in the general Nigerian population.
Other systemic diseases discovered in our patients were anemia (0.8%), with a mixed microcytic and macrocytic picture, and leukemia (0.3%). The objective of the treatment of vitiligo is to satisfy the cosmetic needs of the patients. Most patients were satisfied with cosmetic camouflage, once they and their family had been assured that they did not have leprosy. Interestingly, in the patient with leukemia, the vitiligo was completely cured after pulses of cytotoxic therapy for leukemia.
Discussion
The characteristic appearance of vitiligo on darkly pigmented skin and the social stigmatization of patients in a society in which leprosy is endemic usually encourage patients to seek treatment in specialist units that offer the best available therapy. Thus, the data presented in this report, although hospital-based,probably approximate the true pattern of vitiligo in this region.