1 | INTRODUCTION
Anxiety and depressive disorders are the most common psychopathologies in children and adolescents.1 Alopecia areata (AA) is a common hair disorder characterized by a sudden-onset non-cicatricial but has a great negative effect on cosmetic appearance. Several studies have estimated the prevalence of AA worldwide to be 1%-2%, and in the majority, the first patch presents before the age of 20 years.2 Vitiligo is characterized by the partial or complete absence of melanocytes that cause the development of white macules or patches in various parts of the body.3,4 The worldwide prevalence of vitiligo is estimated to be 0.5%-2%, and approximately 50% of patients experience vitiligo before the age of 20 years.5,6 Since their visibility, chronic and disfiguring nature, and lack of curative therapy, AA and vitiligo may have high psychosocial effects on patients. AA and vitiligo are associated with various psychiatric comorbidities. In different studies, high anxiety and depressive disorder rates have been reported in children and adolescents with AA.7-11 Studies have shown that vitiligo patients suffer more from depression and anxiety.12-14 However, there are only a limited number of studies investigating the relationship between vitiligo and psychiatric state in children and adolescents.15-17
Skin diseases have a negative effect on family life,18-20 and the care of a child with AA or vitiligo may be associated with higher anxiety and depression in their parents than that of healthy children. Unlike other studies, in the current work, children and adolescents with AA and vitiligo and their parents were compared with each other and also with the healthy control group. Therefore, we aimed to identify psychiatric findings in children and adolescent groups with AA and vitiligo and to evaluate the levels of anxiety and depression in their parents. We also aimed to investigate the quality of life (QoL) of patients, and the impact of the disease on their parents.
2 | MATERIAL AND METHOD
2.1 | Study design and subjects
This is a prospective cross-sectional study conducted in our dermatology outpatient clinic between October 2018 and December 2019. The study was approved by the institutional ethical committee and carried out in accordance with the principles of the Declaration of Helsinki. Patients, controls, and their parents, who agreed to participate in the study, provided informed consent.
The study included children and adolescents aged seven to 17 years and their parents. Of the patients, 31 had AA and 29 had vitiligo. In addition, 30 age- and gender-matched healthy controls without any dermatological disease and their parents with a similar education level to that of the patients’ parents were included as a reference group. The following exclusion criteria were used for both the patient and control groups: systemic treatment (systemic steroid, cyclosporin and/or neuropsychiatric drugs) within the last three months prior to the study and any other chronic disease.
2.2 | Demographic variables and clinical severity
Demographic data (patient age and gender, and parental age and education level) and medical information (disease duration, disease severity, and presence of stressful life events within the past year from the onset of disease) were noted in separate forms for the patients. In addition, through a clinical examination, the Severity of Alopecia Tool (SALT) score21 was calculated for the patients with AA, and the Vitiligo Area Severity Index (VASI)22 for those with vitiligo.
The questionnaires explained below were administered in a single interview. The patients and controls completed the Revised Child Anxiety and Depression Scales-Child version (RCADS-C), and their parents completed the parent version (RCADS-P) to support the results of the child version. The parents also completed the Beck Anxiety Inventory (BAI) and Beck Depression Inventory (BDI). Lastly, the Children’s Dermatology Life Quality Index (CDLQI) scale was completed by the patients, and the Dermatological Family Impact Scale (DeFIS) by their parents.
2.3 | Scales on psychological parameters and QoL
CDLQI is a four-point Likert scale that evaluates the state of the patients and can be used in children aged four to 17 years. Higher scores indicate a greater level of deterioration in QoL. In this study, we used the Turkish version of this scale, for which validity and reliability studies have been previously conducted.23
RCADS-C and RCADS-P are self-report questionnaires, each containing 47 items designed to assess DSM-IV depression and anxiety disorders in children and adolescents. Response options are based on four-point Likert scales. Both versions have six subscales [separation anxiety disorder (SAD), social phobia (SP), obsessive-compulsive disorder (OCD), panic disorder (PD), generalized anxiety disorder (GAD), and major depressive disorder (MDD)] and provide a total anxiety score (sum of the score in five anxiety scales) and a total internalizing score (sum of the six scores in subscales).24 In this study, we used the Turkish versions of these questionnaires. The validity and reliability studies of the Turkish versions have been previously conducted.25,26
DeFIS is a 15-item, five-choice response scale to investigate how the family QoL of patients with chronic dermatosis has been affected within the last month and produces a score of 0-4. Higher scores indicate greater impairment in QoL. The scale was developed for the Turkish society by Turan et al, and the validity and reliability studies have been undertaken by the same authors.27
BAI is a 21-item self-report scale that was used to measure parents’ anxiety levels in this study. The items include symptoms of anxiety and higher total scores indicating greater anxiety levels. BAI was previously adapted to the Turkish society, and the Turkish version of the scale was in the current study.28
BDI is a 21-item self-report scale that was used to measure the level of depression in parents. There are four statements for each symptom, and a higher total score indicates a higher level of depression. The validity and reliability studies of the Turkish adaptation of the 1979 version of BDI have been undertaken.29,30
2.4 | Statistical analysis
As the statistical method, descriptive analyses (frequency distributions, percentage, mean, and standard deviation) were used. For the analysis of continuous data, conformance to normal distribution was checked using the Kolmogorov-Smirnov test. For the data that were normally distributed, the comparison of more than two groups was undertaken with ANOVA and the post hoc Bonferroni test and the comparison of two groups using the t-test.
In the absence of normal distribution, Kruskal-Wallis and MannWhitney U tests were performed, the chi-square test was used for discrete data, and Fisher’s exact test was conducted depending on the data compatibility. Relationships were investigated by the
TABLE 1 Characteristics of patients and controls
Spearman rho correlation coefficient. The results were evaluated at the 95% confidence interval and P < .05 significance level.
3 | RESULTS
3.1 | Demographic and clinical characteristics of the study groups
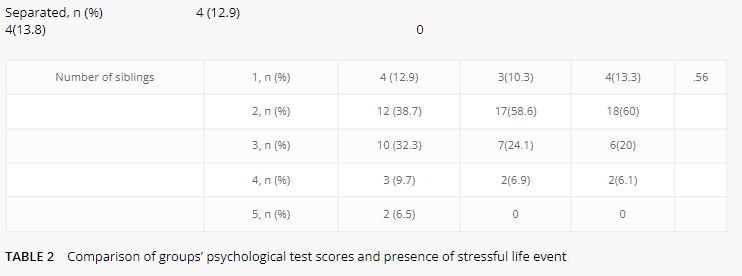
Thirty-one patients with AA, 29 patients with vitiligo, and 30 age- and gender-matched controls were included in the study. The mean (± standard deviation) ages of the in the AA, vitiligo, and control groups were 12.5 ± 3.6, 13 ± 3, and 12.6 ± 3.1 years, respectively. There was no statistically significant difference between the patient and control groups in terms of age, gender, number of siblings, parental education level, and parental marital status (Table 1). All patients with AA had the patchy type, and their mean SALT score was 6.3 ± 13.1. In the vitiligo group, the type of disease was vulgaris in 51.7% (n = 15), focal in 44.8% (n = 13), and segmental in 3.4% (n = 1). The mean VASI score of the vitiligo group was 3.6 ± 7.4. The mean disease duration was 6.5 ± 15.5 (range, 1-84) months in the AA group and 31.4 ± 35.5 (range, 2-132) months in the vitiligo group.
The difference between the AA, vitiligo, and control groups in terms of the presence of stressful life events was statistically
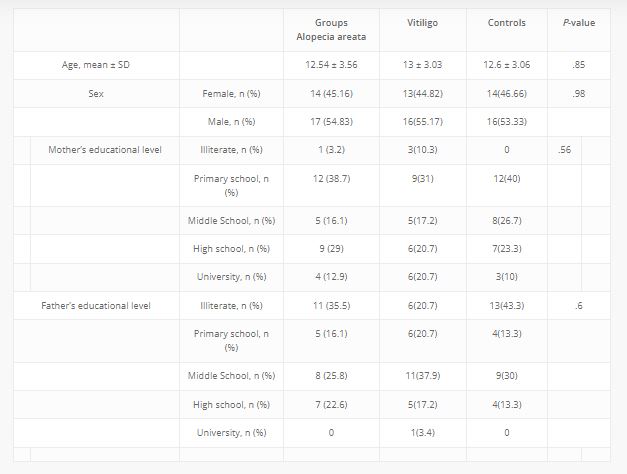
Parental marital status Married, n (%) 27 (87.1) 25(86.2) 30(100) .11
Separated, n (%) 4 (12.9) 4(13.8) 0
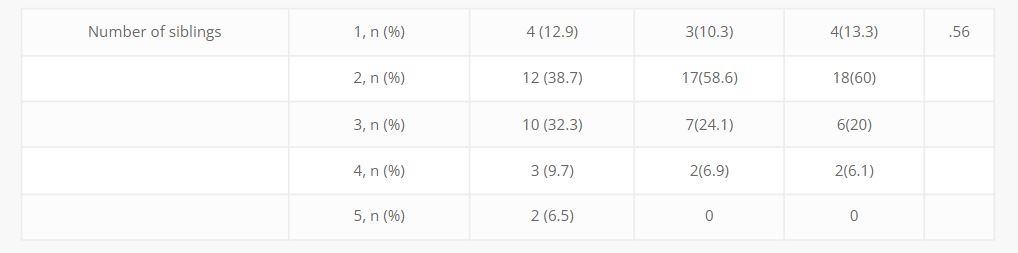
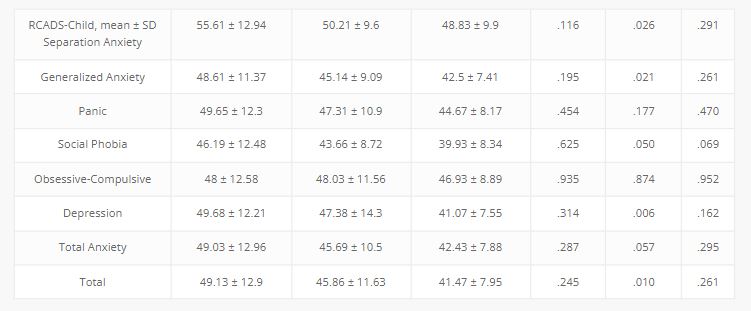
TABLE 2 Comparison of groups’ psychological test scores and presence of stressful life event
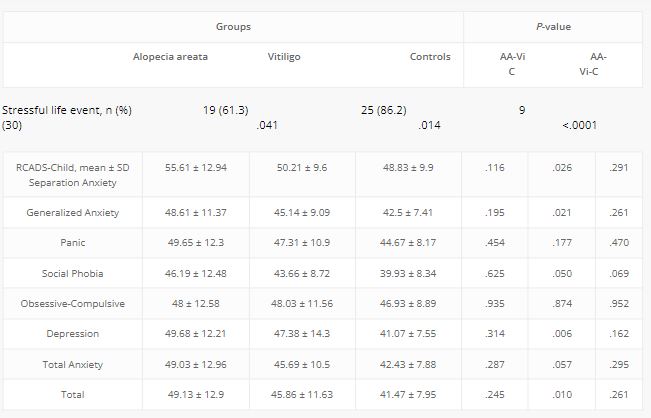
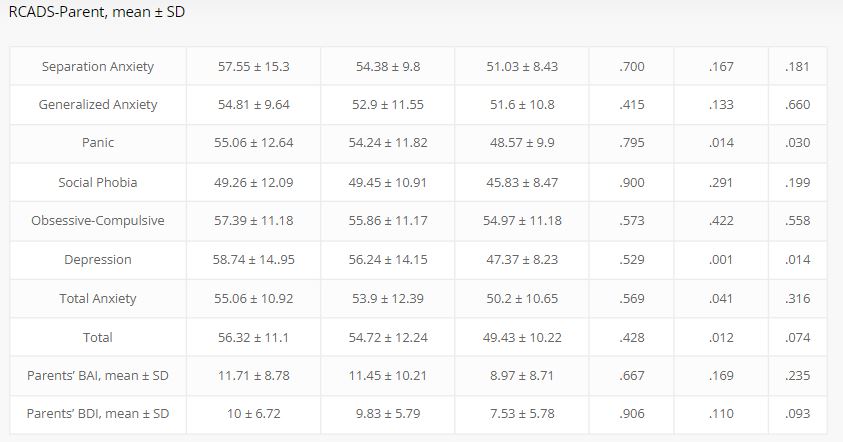
Abbreviations: AA, Alopecia Areata; Vi, Vitiligo; C, Controls; BAI, Beck Anxiety Inventory; BDI, Beck Depression Inventory; RCADS-Child, Revised Child Anxiety and Depression Scales, Child Version; RCADS-Parent, Revised Child Anxiety and Depression Scales, Parent Version.
significant (P < .0001). Furthermore, this parameter was statistically significantly higher in the vitiligo group compared to the AA and control groups (P = .014 and P < .0001, respectively) (Table 2).
Abbreviations: AA, Alopecia Areata; Vi, Vitiligo; C, Controls; BAI, Beck Anxiety Inventory; BDI, Beck Depression Inventory; RCADS-Child, Revised Child Anxiety and Depression Scales, Child Version; RCADS-Parent, Revised Child Anxiety and Depression Scales, Parent Version.
significant (P < .0001). Furthermore, this parameter was statistically significantly higher in the vitiligo group compared to the AA and control groups (P = .014 and P < .0001, respectively) (Table 2).
1.1 | Evaluation of the scales related to psychological parameters and QoL
The mean CDLQI score was 5.1 ± 5.13 (0-22) in the AA group and
2.76 ± 2.39 (0-8) in the vitiligo group; the mean DeFIS score was 12.19 ± 11 (0-54) in the AA group and 14.45 ± 9.33 (0-45) in the vitiligo group, indicating no significant difference (P = .245, P = .102, respectively).
In the AA group, the scores in the RCADS-C subscales of SAD
(P = .026), GAD (P = .021), SP (P = .049) and MDD (P = .006), and the total (P = .010) scores were significantly higher compared to the control group. According to the results of RCADS-P, the scores in the subscales of PD (P = .015) and MDD (P = .001), and the total anxiety (P = .041) and total (P = .012) scores were significantly higheramong the patients in the AA group compared to the control group (Table 2). While there was no significant difference in the vitiligo group in terms of the RCADS-C scale scores, according to RCADS-P, the PD (P = .030) and MDD (P = .014) subscores of the patients were significantly higher than the controls (Table 2). There was no significant difference between the AA and vitiligo groups in relation to the RCADS-C and RCADS-P scores. Similarly, no significant difference was observed between the AA, vitiligo, and control groups in terms of the parents’ BAI and BDI scores (Table 2).
Concerning the relationship between disease severity and total anxiety and depression scores, in the AA group, the SALT score had a positive correlation with RCADS-C depression (P = .014) and total anxiety (P = .032) and RCADS-P depression (P = .023) and total anxiety (P = .014) scores. However, in this group, no significant correlation was detected between the parents’ BAI (P = .321) and BDI (P = .161) scores. In the vitiligo group, there was no significant correlation between the VASI score and the total anxiety and depression scores, but the VASI score was found to be positively correlated with the RCADS-P SAD score (P = .048). There was no significant relationship between the parents’ BAI (P = .829) and BDI (P = .981) scores in the vitiligo group (Table 3).
In the AA group, the CDLQI score was positively correlated with the scores obtained from SALT (P = .008), RCADS-C depression (P = .012) and total anxiety (P = .041), DeFIS (P = .010), parental BAI (P = .011), and parental BDI (P = .022). In the vitiligo group, the CDLQI score had a positive correlation with the scores of RCADS-C depression (P = .001) and total anxiety (P = .007), and RCADS-P
TABLE 3 Correlation between SALT,
VASI, CDLQI, DeFIS, RCADS-C, RCADS-P, BAI, and BDI scores in patients with alopecia areata and vitiligo (Spearman rho)
| Separation Anxiety | .383* | .271 | .195 | .256 | .350 | .489** | |||
| Generalized Anxiety | .387* | .307 | .409* | −.132 | .299 | .361 | |||
| Panic | .381* | .342 | .431* | .104 | .481** | .377* | |||
| Social Phobia | .236 | .317 | .313 | −.114 | .281 | .162 | |||
| Obsessive-Compulsive | .428* | .370* | .330 | .197 | .571** | .477** | |||
| Depression | .438* | .443* | .377* | .164 | .589** | .325 | |||
| Total Anxiety | .386* | .370* | .378* | .067 | .491** | .455* | |||
| Total | .448* | .445* | .425* | .102 | .570** | .440* | |||
| RCADS-ParentSeparation Anxiety | .292 | .310 | .242 | .371* | .230 | .574** | |||
| Generalized Anxiety | .455* | .365* | .495** | .061 | .318 | .368* | |||
| Panic | .157 | .127 | .372* | .142 | .310 | .396* | |||
| Social Phobia | .398* | .169 | .428* | .096 | .167 | .203 | |||
| Obsessive-Compulsive | .382* | .336 | .482** | .238 | .344 | .688** | |||
| Depression | .407* | .228 | .400* | −.003 | .383* | .394* | |||
| Total Anxiety | .435* | .309 | .553** | .144 | .332 | .462* | |||
| Total | .454* | .331 | .522** | .053 | .389* | .424* | |||
| Parents’ BAI | .184 | .452* | .515** | −.042 | .169 | .262 | |||
| Parents’ BDI | .258 | .410* | .643** | −.005 | .255 | .185 | |||
| SALT | .466** | .602** | |||||||
| VASI | .048 | .184 | |||||||
| CDLQI | .466** | .455* | .048 | .130 | |||||
| DeFIS | .602** | .455* | .184 | .130 | |||||
Abbreviations: BAI, Beck Anxiety Inventory; BDI, Beck Depression Inventory; CDLQI, Children’s
Dermatology Life Quality Index; DeFIS, Dermatological Family Impact Scale; RCADS-Child, Revised Child Anxiety and Depression Scales, Child Version; RCADS-Parent, Revised Child Anxiety and Depression Scales, Parent Version; SALT, Severity of Alopecia Tool; VASI, Vitiligo Area Severity
Index.
*P < .05.
**P < .01.
depression (P = .040); however, CDLQI did not have a significant relationship with parental BAI (P = .379), parental BDI (P = .183), VASI (P = .804), and DeFIS (P = .500) (Table 3).
In the AA group, the DeFIS score had a positive correlation with the SALT score (P < .0001), the RCADS-C depression (P = .037) and total anxiety (P = .036) scores, the RCADS-P depression (P = .026) and total anxiety (P = .001) scores, the parental BAI score (P = .03), and the parental BDI score (P < .0001). In the vitiligo group, the DeFIS score was positively correlated with the scores of RCADS-C total anxiety (P = .013), and RCADS-P depression (P = .035) and total anxiety (P = .012); however, no significant correlation was observed between the DeFIS score and the parental BAI (P = .169), parental BDI (P = .337), and VASI (P = .340) scores (Table 3).
2 | DISCUSSION
Psychiatric symptoms are very common in dermatology patients, and an undetected psychiatric disorder can significantly reduce the patient’s QoL since it can delay treatment or recovery. We designed this study to better understand the impact of AA and vitiligo on children and their parents. Therefore, we have attempted to study the dimensions of anxiety disorders, that is, SAD, SP, GAD, OCD, and PD. Furthermore, in the current study, the anxiety and depression scales were directly evaluated in addition to the DeFIS scale, which indirectly measures the psychological status of the parents. Present results suggest differences between AA and vitiligo pediatric patients. The presence of stressful life events before the onset of both AA and vitiligo in the pediatric group and emphasized its greater importance for the latter. In addition, anxiety symptoms were more common in AA patients than those with vitiligo.
In a study by Bilgiç et al, AA was shown to have a positive correlation with higher state and trait anxiety and depression scores in children.11 In another study examining children with AA aged nine to 11 years, the patients were found to have significantly higher levels of psychopathology than the controls.7 In our study, we observed a significant difference between the pediatric patients with AA and the control group in terms of the RCADS-C subscales scores in SAD, GAD, SP, and depression, as well as the total scale score, which contributes to and supports previous research. In addition, PD and total anxiety scores were significantly higher in children with AA in the RCADS-P scale. While no significant difference was found in any of the subscales of RCADS-C in the evaluation of vitiligo patients, according to RCADS-P, the PD and depression scores of the patients in the vitiligo group were significantly higher compared to the control parents. The results of studies investigating depression and anxiety scores in patients with vitiligo are variable. In a study evaluating children and adolescents with vitiligo, depression scores were found to be higher than the control groups only in the children (8-12 years) group.16 In another study, children’s level of anxiety and depression symptoms did not significantly differ from the control group.15 However, Ucuz et al reported that the state and trait anxiety scores of children with vitiligo were different from those of the controls.17 The awareness that pediatric patients with alopecia areata and vitiligo are closely related to psychological factors is essential and psychiatric evaluation is important in the management of this population. Such patients should be directed to the child and adolescent psychiatrist, and treatment of the psychological condition can contribute to the medical treatment of dermatological disease.
In a recent study involving the parents of children with vitiligo, the depressive symptoms of the parents were higher than those of the control group, but the authors did not observe a similar link for anxiety symptoms.15 In another study evaluating depression and anxiety symptoms among the carers of patients with different types of dermatoses (vitiligo, atopic dermatitis, and psoriasis), higher levels of anxiety and depression were observed compared to the general population, but no difference was observed between disease groups.18 To the best of our knowledge, there is no study in the literature examining the psychiatric state of the parents of children with AA. In the current study, there was no difference between the anxiety and depression levels of the parents of the patients with AA and vitiligo and those in the control group. Similarly, no significant difference was observed between the vitiligo and AA groups in terms of the DeFIS scores, through which we evaluated the QoL of the parents.
A small number of studies related to the pediatric cases have shown the presence of stressful life events before the onset of AA as a potential trigger of the disease at a rate of 9.5% to 81%.31-34 In studies conducted with children with vitiligo, a history of stressful life events before the onset of the disease was reported at the rates of 48.8%15 and 77%.17 In our study, 61% of children with AA and 86.2% of children with vitiligo had a history of stressful life events in the year prior to the onset of the disease.
There is only one study in the literature that evaluated the severity of AA together with psychological state in children, and the results did not show a significant relationship.11 In contrast, in our study, there was an increase in the depression and anxiety scores of the patients with AA with the increasing severity of the disease, although a positive correlation of disease severity and anxiety and depression levels was not detected for the parents. In the evaluation of patients with vitiligo, Önen et al did not report a relationship between the severity of the disease and anxiety and depression scores in parents or children.15 In other studies in which children and adolescents were examined, no significant relationship was observed between vitiligo severity and anxiety16,17 and depression16 scores. In our study, only the level of SAD was increased with the increasing severity of vitiligo, but there was no positive correlation between disease severity and parental anxiety and depression levels.
In a previous study examining the effect of AA on QoL, it was shown that the QoL of the parents decreased as the severity of the disease increases in the child.35 In a study by Bilgiç et al, AA severity was shown to have a negative effect on the QoL of children.11 Similarly, in our study, impairment in the QoL of both patients and their parents increased with the increasing disease severity in the AA group. However, there are conflicting results in studies investigating the effect of the severity of vitiligo on QoL. For example, in one study, the severity of vitiligo in adolescents was observed to affect QoL negatively16 while two other studies including children and adolescents reported no relationship between QoL and the body surface area36 and vitiligo severity.15 According to another study in which the effect of childhood vitiligo on parents’ QoL was examined, as the area of involvement of vitiligo increased, the parental QoL decreased.37 In the current study, we found no correlation between disease severity and the QoL of patients or parents.
The main limitation of this study is the small sample size and cross-sectional design, and the lack of a structured interview and psychiatric evaluation can be considered as another limitation.
The results of the study indicated that the presence of stressful life events was more common in pediatric patients with vitiligo than those with AA. On the other hand, anxiety symptoms were more prevalent in patients with AA than those with vitiligo. While the severity of AA was correlated with the QoL of the affected children and their parents, there was no such correlation in vitiligo. The QoL of the patients affected the anxiety and depression levels of their parents in the AA group, but not in the vitiligo group. It is important to identify pediatric patients with alopecia areata and vitiligo who need extra psychological support and refer them to the child and adolescent psychiatrist. In conclusion, providing a psychological evaluation and support for both patients and their parents will not only help them better cope with chronic dermatoses that cause cosmetic disorders such as vitiligo and AA but also contribute to the improvement of their QoL.
Image credit: Pexels ,Felix Mejica



